Rib Head Chondrosarcoma associated with Olliers Disease – A Rare Differential for Paraparesis
Upadhyaya S.1, Nair R.2*, Kumar V.3, Aadhav S.4, Shetty A.5
DOI:
1 Sunil Upadhyaya, Associate Professor, Department of Neurosurgery, Kasturba Medical College, Manipal university, Manipal, Karnataka, India.
2* Rajesh Nair, Neurosurgery Registrar, Department of Neurosurgery, Kasturba Medical College, Manipal university, Manipal, Karnataka, India.
3 Vinod Kumar, Associate Professor, Department of Neurosurgery, Kasturba Medical College, Manipal university, Manipal, Karnataka, India.
4 Swapnil Aadhav, Neurosurgery Registrar, Department of Neurosurgery, Kasturba Medical College, Manipal university, Manipal, Karnataka, India.
5 Arjun Shetty, Professor and Head, Department of Neurosurgery, Kasturba Medical College, Manipal university, Manipal, Karnataka, India.
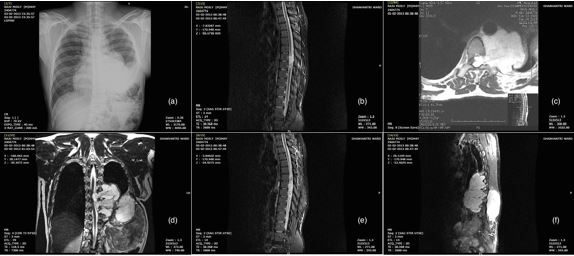
Olliers disease is a non-familial condition affecting 1:100000 (1,2). It is characterized by the presence of multiple enchondromas affecting small tubular bones of the hands, feet and other tubular long bones and flat bones. Malignant transformation of these enchondromas is as high as 5 – 50% (1,2). While cases of de novo chondrosarcomas involving the vertebral body pedicles causing cord compression and neurological deficit have been well documented. We present a rare case of Olliers disease with chondrosarcoma of the rib head who presented with paraparesis secondary to extradural cord compression with intracanalicular extension.
Keywords: Olliers Disease, Chondrosarcoma, Enchondromas, Chondrosarcomas
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Neurosurgery Registrar, Department of Neurosurgery, Kasturba Medical College, Manipal university, Manipal, Karnataka, India. Email:  |
Sunil Upadhyaya, Rajesh Nair, Vinod Kumar, Swapnil Aadhav, Arjun Shetty, Rib Head Chondrosarcoma associated with Olliers Disease – A Rare Differential for Paraparesis. Biomed Rev J Basic Appl Med Sci. 2021;8(1):119-122. Available From http://www.biomedicalreview.in/rib-head-chondrosarcom-associated-olliers-disease-rare-differential-for-paraparesis-case-report |
 |
 ©
©