Overlooked Etiologies of Childhood (0-59 Months) Gastro-Enteritis in a Semi Urban Community
René Fotsing Kwetche P.1*, Gamwo Dongmo S.2, Ngaha A.3, Kaba K.4, Pulchérie Tamatcho Kweyang B.5, Kaptué L.6
DOI:
1* Pierre René Fotsing Kwetche, Institut Supérieur des Sciences de la Santé de Bangangté, Université des Montagnes, Bangangté, Cameroon.
2 Sandrine Gamwo Dongmo, Cliniques Universitaires des montagnes, Bangangté, Cameroon.
3 Augustin Ngaha, Cliniques Universitaires des montagnes, Bangangté, Cameroon.
4 Kourouma Kaba, Université des Montagnes, Bangangté, Cameroon.
5 Blandine Pulchérie Tamatcho Kweyang, Faculty of Science, University of Yaoundé I, Yaoundé, Cameroon.
6 Lazare Kaptué, Faculty of Science, Université des Montagnes, Bangangté, Cameroon.
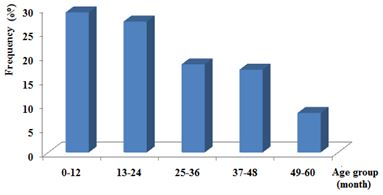
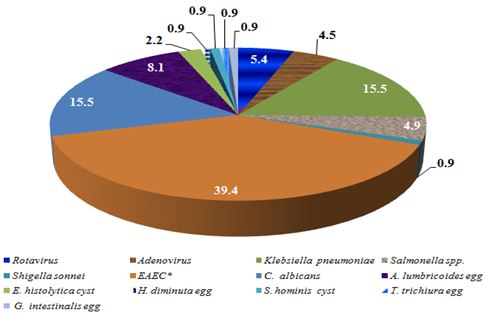
The present study aimed at investigating protozoan, bacterial, fungal and viral (rotavirus, adenovirus) etiologies of diarrhea amongst children aged 0 through 59 months and identifying a few factors likely to influence prevalence rates of this disorder in Bangangté-Cameroon. A questionnaire was designed to gather pieces of information on life style during specimen collection. Microbial screening was conducted on stools specimens according to standard protocols for all microbes. Out of total of 200 stool samples subjected to laboratory examination 64 % were elucidated. In decreasing frequencies, outstanding etiologies included enteroagregative E. coli (EAEC, 39.4%), Candida albicans and Klebsiella pneumonia (15.5% each), Ascaris lumbricoides (8.1%), rotavirus and adenovirus (5.4% and 4.5%, respectively). Screening for EAEC and Klebseilla is not a usual exercise because their role in diarrhea was ignored so far setting. For most of these pathogens, detection rates were associated with age of candidate. Natural protection appeared to increase rapidly against C. albicans and rotavirus. It was also observed that a large number of parents (66.7%) do normally not report their children cases to health facility. When they were appropriately informed, however, number of reported cases could be ten times higher, consistent with crucial role of education in preventing childhood diarrhea.
Keywords: Childhood diarrhea, Klebsiella, EAEC, Viruses
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , , Institut Supérieur des Sciences de la Santé de Bangangté, Université des Montagnes, Bangangté, , Cameroon. Email:  |
Pierre René Fotsing Kwetche, Sandrine Gamwo Dongmo, Augustin Ngaha, Kourouma Kaba, Blandine Pulchérie Tamatcho Kweyang, Lazare Kaptué, Overlooked Etiologies of Childhood (0-59 Months) Gastro-Enteritis in a Semi Urban Community. Biomed Rev J Basic Appl Med Sci. 2020;7(1):67-74. Available From http://www.biomedicalreview.in/overlooked-etiologies-childhood-0-59-months-gastro-enteritis-semi-urban-community-research-article |
 |
 ©
©