Cleidocranial Dysplasia: A Case Report
Kumar L.K S.1, Menon.P V.2*
DOI:
1 Surej Kumar L.K, MDS Consultant, Oral & Maxillofacial Surgery, Kerala Institute of medical sciences (KIMS) Hospital, Trivandrum, Kerala, India.
2* Varun Menon.P, Trainee, Oral & Maxillofacial Surgery, Kerala Institute of medical sciences (KIMS) Hospital, Trivandrum, Kerala, India.
Cleidocranial dysplasia (CCD) is a rare autosomal dominant disorder. This congenital defect is characterized by hypoplastic or absent clavicles, delayed skeletal development .Along with hypoplasia of orofacial and skeletal structures the condition is also reported to have multiple supernumerary teeth, retained deciduous dentition, non-eruption of permanent tooth. We report a case of CCD in a 26 year-old female who had classical diagnostic feature.
Keywords: Cleidocranial dysplasia, multiple missing tooth, absence of clavicles
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Trainee, Oral & Maxillofacial Surgery, Kerala Institute of medical sciences (KIMS) Hospital, Trivandrum, Kerala, India. Email:  |
Surej Kumar L.K, Varun Menon.P, Cleidocranial Dysplasia: A Case Report. Biomed Rev J Basic Appl Med Sci. 2019;6(1):42-45. Available From http://www.biomedicalreview.in/cleidocranial-dysplasia-a-case-report |
 |
 ©
©  Fig 1: Showing the Intra oral Picture
Fig 1: Showing the Intra oral Picture Fig 2: Clubbing of the digits
Fig 2: Clubbing of the digits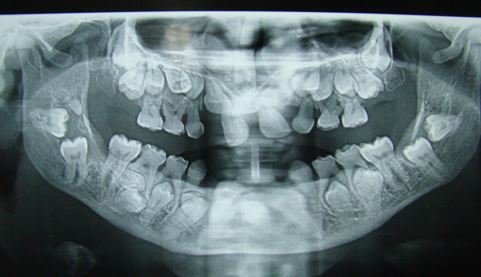 Fig 3: OPG showing multiple impacted tooth and retained deciduous tooth
Fig 3: OPG showing multiple impacted tooth and retained deciduous tooth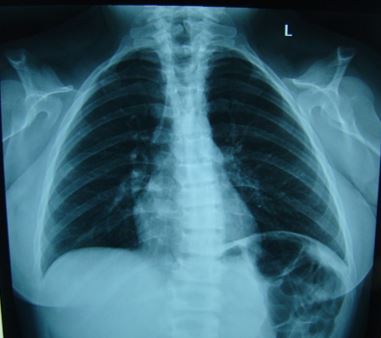 Fig 4: Chest X-ray (PA view) showing bilateral absence of clavicle
Fig 4: Chest X-ray (PA view) showing bilateral absence of clavicle